Login
Welcome back! Please enter your details.
or
Don't have an account? Register here
Create Account
Join MedMentorEdu and start your medical journey.
or
Already have an account? Login here
Enhance your knowledge with our comprehensive guide and curated study materials.
Milk is a complete biological nutrition fluid designed for neonatal survival.
Water: ~87%
Proteins: ~1–1.5%
Fat: ~3–5%
Lactose: ~7%
Minerals: ~0.2%
Lactose (major sugar)
Provides energy
Enhances calcium absorption
Casein
Lactalbumin
Lactoglobulin
Immunoglobulins (IgA)
Human milk has:
More whey protein
Less casein compared to cow’s milk
Triglycerides
Essential fatty acids
DHA (brain development)
Calcium
Phosphorus
Iron (low quantity but highly bioavailable)
IgA
Lactoferrin
Lysozyme
Oligosaccharides (prevent bacterial adhesion)

4
Easily digestible
Anti-infective
Promotes gut microbiota
Lower allergy risk
Colostrum is the first milk produced after delivery (first 3–5 days).
Thick, yellowish fluid.
Higher:
Protein
Immunoglobulin (especially IgA)
Vitamin A
Lower:
Fat
Lactose

4
Passive immunity
Laxative effect (meconium clearance)
Prevents neonatal jaundice
Clear, colorless fluid around brain and spinal cord.
Produced by choroid plexus.
Rate:
≈ 500 mL/day
Total volume:
≈ 150 mL
Lower:
Protein
Glucose (about 2/3 plasma)
Potassium
Higher:
Chloride

4
Protein: 15–45 mg/dL
Glucose: 45–80 mg/dL
Cells: 0–5 lymphocytes/mm³
↑ Protein
↓ Glucose
Neutrophils
Normal glucose
Mild protein rise
Lymphocytes
Fluid surrounding fetus in amniotic sac.
Fetal urine
Fetal lung secretion
Maternal plasma
Protects fetus
Maintains temperature
Allows movement
Prevents adhesion

4
Oligohydramnios → renal agenesis
Polyhydramnios → GI obstruction
Amniocentesis:
Genetic testing
Fetal lung maturity (Lecithin/Sphingomyelin ratio)
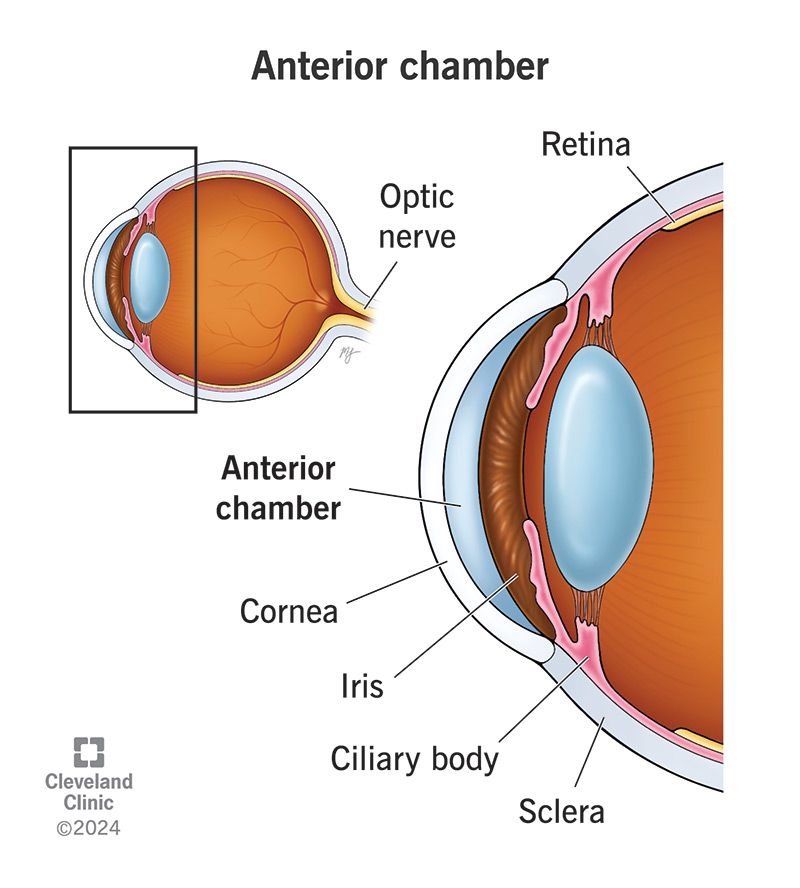
Clear fluid in anterior and posterior chambers of eye.
Produced by ciliary body.
Maintains intraocular pressure
Provides nutrition to cornea & lens
Removes waste

4
Similar to plasma but:
Low protein
Low glucose
Low cells
Glaucoma:
↑ Intraocular pressure
Due to impaired drainage (trabecular meshwork).
Colostrum rich in IgA
CSF glucose ≈ 2/3 plasma
Normal CSF protein low
Amniotic fluid source: fetal urine
Aqueous humor produced by ciliary body
Glaucoma due to impaired aqueous drainage
Clear, colorless fluid surrounding brain and spinal cord.
Produced by choroid plexus in ventricles.
Rate of formation: ≈ 500 mL/day
Total volume in adults: ≈ 150 mL
Turnover: ~3–4 times/day
4
Lateral ventricles → Third ventricle → Aqueduct of Sylvius → Fourth ventricle → Subarachnoid space → Absorbed via arachnoid villi into venous sinuses.
Cushions brain (shock absorber)
Maintains constant intracranial pressure
Nutrient supply & waste removal
Maintains ionic balance for neuronal function
| Parameter | CSF | Plasma |
|---|---|---|
| Protein | Low (15–45 mg/dL) | Higher |
| Glucose | 45–80 mg/dL (~2/3 plasma) | Higher |
| Chloride | Slightly higher | Slightly lower |
| Cells | 0–5 lymphocytes/mm³ | Many |
Low protein due to blood-brain barrier.
↑ Protein
↓ Glucose
Neutrophils
Turbid appearance
Mild ↑ Protein
Normal glucose
Lymphocytes
Xanthochromia
Albuminocytologic dissociation
(↑ protein, normal cells)
Fluid surrounding fetus within amniotic sac.
Volume:
~50 mL at 12 weeks
~800–1000 mL at term

4
Fetal urine (major source in late pregnancy)
Fetal lung secretions
Transudation from maternal plasma
Protects from trauma
Maintains temperature
Allows fetal movement
Prevents cord compression
Helps lung development
Causes:
Renal agenesis
Placental insufficiency
Post-term pregnancy
Risk:
Pulmonary hypoplasia
Causes:
GI obstruction (e.g., esophageal atresia)
Maternal diabetes
Neural tube defects
Most important clinical test:
Assessment of fetal lung maturity.
Lecithin increases with lung maturity.
Sphingomyelin remains constant.
L/S ratio:
<1.5 → Immature lungs
≥2 → Mature lungs
Very high-yield exam point.
Appears late in pregnancy.
Presence indicates lung maturity.
Amniotic fluid + ethanol → shake.
Persistent foam ring = adequate surfactant.
Lamellar bodies contain surfactant.
High count = mature lungs.
Used in hemolytic disease of newborn.
Measured via spectrophotometry (ΔOD450).
Immature lungs → Respiratory Distress Syndrome (RDS).
Due to surfactant deficiency.
Surfactant reduces alveolar surface tension.
Main component:
Dipalmityl phosphatidylcholine (DPPC).
CSF glucose = 2/3 plasma
CSF protein low due to blood-brain barrier
Bacterial meningitis → ↓ glucose, ↑ protein
Amniotic fluid major source late pregnancy → fetal urine
L/S ratio ≥2 indicates lung maturity
Surfactant deficiency → neonatal RDS
CSF protects the brain.
Amniotic fluid protects the fetus.
Surfactant determines the first breath.
Q1. What is the major carbohydrate in human milk?
Lactose.
Q2. What is the main protein fraction in human milk?
Whey proteins (lactalbumin predominates over casein).
Q3. Why is human milk easily digestible?
Lower casein content and higher whey proteins.
Q4. What immunoglobulin is abundant in breast milk?
IgA.
Q5. What is the function of lactoferrin?
Binds iron and inhibits bacterial growth.
Q6. What is colostrum?
First milk secreted during initial 3–5 days after delivery.
Q7. How does colostrum differ from mature milk?
Higher protein and IgA; lower fat and lactose.
Q8. Why is colostrum important for neonate?
Provides passive immunity.
Q9. What is the laxative effect of colostrum useful for?
Expulsion of meconium and prevention of neonatal jaundice.
Q10. Where is CSF produced?
Choroid plexus.
Q11. Daily CSF production rate?
About 500 mL/day.
Q12. Total CSF volume in adults?
Approximately 150 mL.
Q13. What is normal CSF protein level?
15–45 mg/dL.
Q14. What is normal CSF glucose?
45–80 mg/dL (~2/3 plasma glucose).
Q15. Why is CSF protein low?
Blood-brain barrier restricts protein passage.
Q16. What is normal CSF cell count?
0–5 lymphocytes/mm³.
Q17. What happens to CSF glucose in bacterial meningitis?
Decreases.
Q18. What happens to CSF protein in meningitis?
Increases.
Q19. What is albuminocytologic dissociation?
High CSF protein with normal cell count (seen in Guillain–Barré syndrome).
Q20. What is xanthochromia?
Yellow discoloration of CSF due to hemoglobin breakdown (subarachnoid hemorrhage).
Q21. What is the main source of amniotic fluid in late pregnancy?
Fetal urine.
Q22. What is normal amniotic fluid volume at term?
800–1000 mL.
Q23. Functions of amniotic fluid?
Protection, temperature regulation, movement, lung development.
Q24. What is oligohydramnios?
Decreased amniotic fluid.
Q25. Major cause of oligohydramnios?
Renal agenesis.
Q26. What is polyhydramnios?
Increased amniotic fluid.
Q27. Causes of polyhydramnios?
GI obstruction, maternal diabetes, neural tube defects.
Q28. Most important indicator of fetal lung maturity?
Lecithin–sphingomyelin (L/S) ratio.
Q29. What L/S ratio indicates maturity?
≥ 2.
Q30. Why does lecithin increase in late pregnancy?
Increased surfactant production.
Q31. What is the main component of surfactant?
Dipalmityl phosphatidylcholine (DPPC).
Q32. What disease results from surfactant deficiency?
Neonatal respiratory distress syndrome.
Q33. What is phosphatidylglycerol significance?
Presence indicates lung maturity.
Q34. What is foam stability (shake) test?
Test for surfactant presence using ethanol.
Q35. What is lamellar body count?
Measurement of surfactant-containing particles in amniotic fluid.
Q36. What is ΔOD450 used for?
Assessment of fetal hemolysis via bilirubin measurement.
Q37. Where is aqueous humor produced?
Ciliary body.
Q38. Main function of aqueous humor?
Maintains intraocular pressure.
Q39. Why is aqueous humor protein low?
Blood-aqueous barrier restricts protein entry.
Q40. What condition results from impaired drainage?
Glaucoma.
Q41. Through which structure does aqueous humor drain?
Trabecular meshwork into canal of Schlemm.
Q42. Which body fluid has lowest protein concentration?
CSF (among major fluids discussed).
Q43. Which fluid contains high IgA?
Colostrum.
Q44. Which fluid is analyzed for fetal lung maturity?
Amniotic fluid.
Q45. Which fluid maintains brain buoyancy?
CSF.
Q46. Which fluid maintains intraocular pressure?
Aqueous humor.
Q47. Why is CSF glucose measured in meningitis?
Bacteria consume glucose, lowering its level.
Q48. Why is human milk preferred over cow milk?
Better digestibility and immune protection.
Q49. What prevents protein entry into CSF?
Blood-brain barrier.
Q50. What biochemical factor allows neonate’s first breath?
Surfactant production.
CSF glucose = 2/3 plasma
CSF protein low
L/S ratio ≥ 2 = mature lungs
Colostrum rich in IgA
Aqueous humor from ciliary body
Surfactant = DPPC
Body fluids are chemically specialized environments.
Each one is tuned to its purpose — brain protection, fetal development, neonatal immunity, or optical clarity.
A. 50 mL
B. 100 mL
C. 150 mL
D. 500 mL
A. 100 mL
B. 250 mL
C. 500 mL
D. 1000 mL
A. Pia mater
B. Arachnoid villi
C. Choroid plexus
D. Hypothalamus
A. Equal to plasma
B. Half plasma
C. Two-thirds plasma
D. One-third plasma
A. 1–5 mg/dL
B. 15–45 mg/dL
C. 60–100 mg/dL
D. 150 mg/dL
A. High metabolism
B. Dilution
C. Blood-brain barrier
D. Low synthesis
A. Viral meningitis
B. Bacterial meningitis
C. Multiple sclerosis
D. Guillain–Barré syndrome
A. Bacterial meningitis
B. Viral meningitis
C. Guillain–Barré syndrome
D. Tuberculosis
A. Viral infection
B. Subarachnoid hemorrhage
C. Hypoglycemia
D. Tumor
A. Maternal sweat
B. Fetal urine
C. Placenta
D. Liver
A. 200 mL
B. 400 mL
C. 800–1000 mL
D. 2000 mL
A. Esophageal atresia
B. Renal agenesis
C. Maternal diabetes
D. Neural tube defect
A. Renal agenesis
B. GI obstruction
C. Dehydration
D. Hypothyroidism
A. Bilirubin level
B. Protein content
C. L/S ratio
D. Glucose
A. 1
B. 1.5
C. 2 or more
D. 3
A. Cholesterol
B. Phosphatidylcholine
C. Triglyceride
D. Glycogen
A. Albumin
B. Lecithin
C. Cholesterol
D. Hemoglobin
A. Bilirubin
B. Surfactant
C. Glucose
D. Protein
A. Infection
B. Hemolysis
C. Lung maturity
D. Placental failure
A. Glucose
B. Protein
C. Bilirubin
D. Lecithin
A. Sucrose
B. Maltose
C. Lactose
D. Fructose
A. IgG
B. IgM
C. IgA
D. IgE
A. Lower protein
B. Higher fat
C. Higher immunoglobulins
D. Lower vitamins
A. Cow milk
B. Human milk
C. Plasma
D. CSF
A. Digest lactose
B. Bind iron
C. Bind glucose
D. Bind sodium
A. Retina
B. Lens
C. Ciliary body
D. Iris
A. Brain pressure
B. Intraocular pressure
C. Plasma osmolality
D. Blood pressure
A. Increased CSF
B. Decreased protein
C. Impaired aqueous drainage
D. Retinal damage
A. Optic nerve
B. Canal of Schlemm
C. Retina
D. Lens
A. Lower than plasma
B. Equal to plasma
C. Slightly higher than plasma
D. Absent
A. Nutrient storage
B. Oxygen transport
C. Shock absorption
D. Fat digestion
A. 50–100
B. 10–20
C. 0–5
D. 100–200
A. Antibody
B. Immunity
C. Energy
D. Sodium
A. Clear
B. Turbid
C. Colorless
D. Yellow
A. Very low
B. Normal
C. Absent
D. High
A. CSF removal
B. Lung maturity assessment
C. Eye pressure
D. Milk analysis
A. Digestion
B. Brain nutrition
C. Protection of fetus
D. Immunity
A. Sodium
B. Chloride
C. Protein
D. Water
A. Osmotic pressure
B. Surface tension
C. Blood pressure
D. Sodium
A. High fat
B. Laxative effect
C. Sodium
D. Protein
C
C
C
C
B
C
B
C
B
B
C
B
B
C
C
B
B
B
C
C
C
C
C
B
B
C
B
C
B
C
C
C
C
B
B
B
C
C
B
B
These fluids are small-volume, high-importance systems.
Miss one biochemical parameter, and diagnosis shifts entirely.
(CSF, Amniotic Fluid, Fetal Maturity, Milk, Colostrum, Aqueous Humor)
Q1. Where is CSF produced?
Choroid plexus of ventricles.
Q2. Daily CSF production?
About 500 mL per day.
Q3. Total CSF volume in adults?
Approximately 150 mL.
Q4. Normal CSF protein level?
15–45 mg/dL.
Q5. Why is CSF protein low?
Due to blood-brain barrier restriction.
Q6. CSF glucose level compared to plasma?
About two-thirds of plasma glucose.
Q7. Normal CSF cell count?
0–5 lymphocytes/mm³.
Q8. What happens to CSF glucose in bacterial meningitis?
It decreases.
Q9. What happens to CSF protein in meningitis?
It increases.
Q10. What is albuminocytologic dissociation?
High protein with normal cell count (seen in Guillain–Barré syndrome).
Q11. What is xanthochromia?
Yellow discoloration of CSF due to hemoglobin breakdown.
Q12. Why is chloride slightly higher in CSF?
Due to active transport and ionic regulation across blood-brain barrier.
Q13. Main source of amniotic fluid in late pregnancy?
Fetal urine.
Q14. Normal volume at term?
800–1000 mL.
Q15. Main functions of amniotic fluid?
Protection, movement, lung development, temperature control.
Q16. What is oligohydramnios?
Decreased amniotic fluid.
Q17. Common cause of oligohydramnios?
Renal agenesis.
Q18. What is polyhydramnios?
Excess amniotic fluid.
Q19. Cause of polyhydramnios in fetal GI obstruction?
Failure of fetus to swallow amniotic fluid.
Q20. What is amniocentesis?
Sampling of amniotic fluid for diagnostic purposes.
Q21. Most important test for lung maturity?
Lecithin–sphingomyelin (L/S) ratio.
Q22. What L/S ratio indicates maturity?
Two or more.
Q23. Why does lecithin increase near term?
Due to increased surfactant synthesis.
Q24. Main component of pulmonary surfactant?
Dipalmityl phosphatidylcholine.
Q25. Disease due to surfactant deficiency?
Neonatal respiratory distress syndrome.
Q26. What does presence of phosphatidylglycerol indicate?
Lung maturity.
Q27. What is the foam stability (shake) test?
A test for surfactant presence using ethanol.
Q28. What does ΔOD450 measure?
Bilirubin in amniotic fluid (hemolytic disease).
Q29. Major carbohydrate in human milk?
Lactose.
Q30. Major immunoglobulin in colostrum?
IgA.
Q31. Why is colostrum yellow?
High protein and beta-carotene content.
Q32. How does colostrum differ from mature milk?
Higher protein and antibodies, lower fat and lactose.
Q33. What is the function of lactoferrin?
Binds iron and inhibits bacterial growth.
Q34. Why is human milk preferred over cow’s milk?
Better digestibility and immune protection.
Q35. What type of protein predominates in human milk?
Whey proteins.
Q36. Where is aqueous humor produced?
Ciliary body.
Q37. Function of aqueous humor?
Maintains intraocular pressure and nourishes cornea and lens.
Q38. Why is protein low in aqueous humor?
Due to blood-aqueous barrier.
Q39. Through which structure does aqueous humor drain?
Trabecular meshwork into canal of Schlemm.
Q40. What happens if drainage is impaired?
Glaucoma.
Q41. Which fluid has lowest protein concentration?
CSF.
Q42. Which fluid protects brain from mechanical injury?
CSF.
Q43. Which fluid helps fetal lung development?
Amniotic fluid.
Q44. Which test predicts neonatal respiratory function?
L/S ratio.
Q45. Why does bacterial meningitis lower CSF glucose?
Bacteria consume glucose.
Q46. Why is colostrum important immediately after birth?
Provides passive immunity.
Q47. What prevents large proteins from entering CSF?
Blood-brain barrier.
Q48. Why does surfactant prevent alveolar collapse?
Reduces surface tension.
Q49. Which fluid maintains optical clarity of anterior chamber?
Aqueous humor.
Q50. Which fluid change suggests hemolytic disease of fetus?
Raised bilirubin in amniotic fluid.
Get the full PDF version of this chapter.