Login
Welcome back! Please enter your details.
or
Don't have an account? Register here
Create Account
Join MedMentorEdu and start your medical journey.
or
Already have an account? Login here
Enhance your knowledge with our comprehensive guide and curated study materials.
Total body calcium ≈ 1–1.2 kg.
Distribution:
99% in bone (as hydroxyapatite)
1% in ECF and cells
Serum calcium (normal):
8.5–10.5 mg/dL
Forms in plasma:
Ionized (active) ~50%
Protein-bound ~40%
Complexed ~10%
Ionized calcium is physiologically active.
4
Muscle contraction
Nerve transmission
Blood clotting
Enzyme activation
Hormone secretion
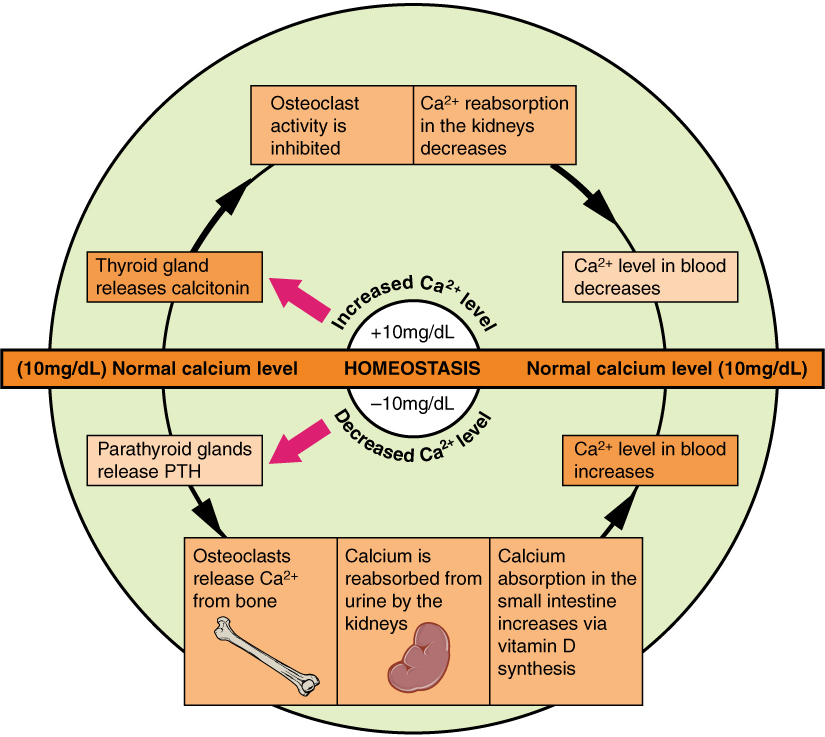
Maintained by:
Parathyroid hormone (PTH)
Vitamin D (Calcitriol)
Calcitonin
Three organs involved:
Bone
Kidney
Intestine
Secreted by:
Parathyroid glands.
Stimulus:
Low serum calcium.
Stimulates osteoclast activity indirectly → releases calcium.
Increases calcium reabsorption
Decreases phosphate reabsorption
Stimulates 1α-hydroxylase → ↑ Calcitriol
Indirectly increases calcium absorption via calcitriol.
Net effect:
Raises serum calcium.
4
Secreted by:
Parafollicular (C) cells of thyroid.
Stimulus:
High serum calcium.
Action:
Inhibits osteoclast activity.
Net effect:
Lowers serum calcium.
Clinical importance limited in adults.
Serum calcium > 10.5 mg/dL.
Common causes:
Hyperparathyroidism
Malignancy
Vitamin D excess
Immobilization
Mnemonic:
“Bones, stones, groans, psychiatric overtones”
Bone pain
Kidney stones
Abdominal pain
Confusion
ECG:
Short QT interval.
Serum calcium < 8.5 mg/dL.
Causes:
Hypoparathyroidism
Vitamin D deficiency
Chronic kidney disease
Tetany
Muscle cramps
Seizures
Positive Chvostek sign
Positive Trousseau sign
ECG:
Prolonged QT interval.
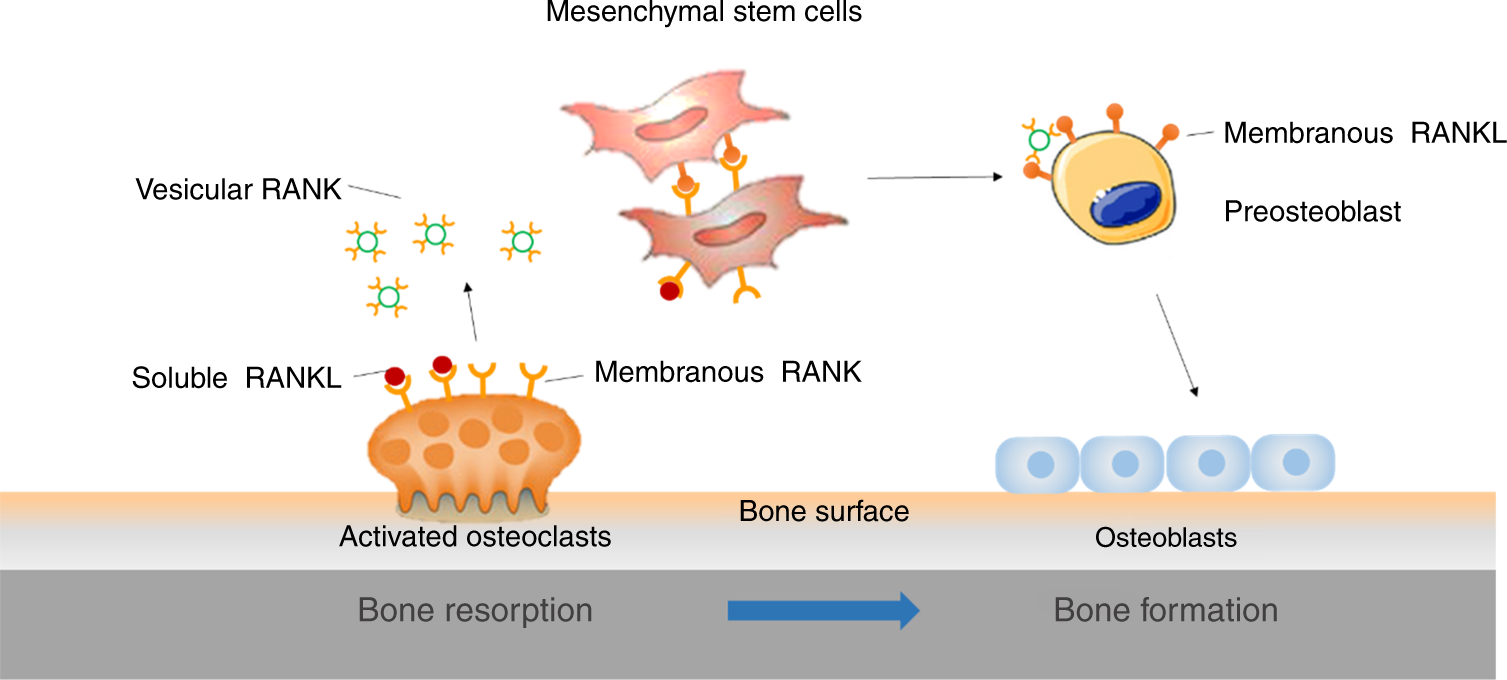
Bone is dynamic.
Two main cell types:
Osteoblasts (build bone)
Osteoclasts (resorb bone)
Bone remodeling is continuous.
Collagen (organic)
Hydroxyapatite (inorganic)
PTH:
Promotes bone resorption.
Calcitriol:
Promotes mineralization (but supports resorption if calcium low).
Calcitonin:
Inhibits resorption.
Low bone mass.
Defective mineralization.
Bone resorption.
4
Low calcium → ↑ PTH → ↑ bone resorption + ↑ calcitriol
High calcium → ↑ calcitonin
Ionized calcium is active.
Albumin affects total calcium but not ionized calcium.
Corrected calcium formula:
Corrected Ca = Measured Ca + 0.8 × (4 − serum albumin)
Examiner favorite.
PTH ↑ calcium, ↓ phosphate
Calcitonin ↓ calcium
Vitamin D ↑ calcium absorption
Hypercalcemia → short QT
Hypocalcemia → tetany
99% calcium in bone
Calcium metabolism is a balancing act between bone and blood.
Bone is storage. Blood is function.
Serum Alkaline Phosphatase (ALP)
Osteocalcin
Procollagen type 1 N-terminal peptide (P1NP)
Raised in:
Rickets
Osteomalacia
Hyperparathyroidism
Paget disease
Urinary hydroxyproline
C-terminal telopeptide (CTX)
N-terminal telopeptide (NTX)
High in:
Osteoporosis
Hyperparathyroidism


4
Normal serum phosphate:
2.5–4.5 mg/dL
Major component of:
Hydroxyapatite
ATP
Nucleic acids
Phospholipids
Controlled by:
PTH (decreases phosphate reabsorption in kidney)
Vitamin D (increases absorption)
Causes:
Hyperparathyroidism
Vitamin D deficiency
Refeeding syndrome
Causes:
Renal failure
Hypoparathyroidism
Normal:
1.7–2.2 mg/dL
Functions:
Cofactor for ATP-dependent enzymes
Neuromuscular stability
PTH secretion
Causes:
Alcoholism
Diarrhea
Diuretics
Effects:
Tetany
Arrhythmia
Hypocalcemia (due to impaired PTH)
Derived from sulfur-containing amino acids:
Methionine
Cysteine
Functions:
Disulfide bonds in proteins
Detoxification reactions (sulfation)
Structure of keratin
Deficiency rare.
Total body iron:
3–4 g.
Distribution:
Hemoglobin (major share)
Myoglobin
Ferritin (storage)
Transferrin (transport)
4
Site:
Duodenum.
Two forms:
Heme iron (better absorbed)
Non-heme iron (Fe³⁺)
Vitamin C enhances absorption.
Regulatory hormone:
Hepcidin (from liver)
Hepcidin blocks iron release from enterocytes.
Causes:
Chronic blood loss
Poor diet
Pregnancy
Lab findings:
Low hemoglobin
Low serum ferritin
High TIBC
Low serum iron
Peripheral smear:
Microcytic hypochromic anemia.
Iron overload disorder.
Types:
Primary (genetic)
Secondary (transfusion-related)
Liver cirrhosis
Diabetes
Bronze skin pigmentation
Cardiomyopathy
Lab:
High ferritin
High serum iron
Low TIBC
PTH:
↑ Calcium
↓ Phosphate
Magnesium:
Required for PTH release.
Iron deficiency:
Low ferritin first.
Hemochromatosis:
High ferritin + high transferrin saturation.
ALP → Bone formation
CTX → Bone resorption
Phosphate partners calcium
Magnesium stabilizes nerves
Iron transported by transferrin
Ferritin reflects storage
Hepcidin blocks iron absorption
Total body copper ≈ 100 mg.
Transported in plasma by ceruloplasmin.
Functions:
Iron metabolism
Collagen cross-linking
Melanin synthesis
Antioxidant defense
Ceruloplasmin (ferroxidase)
Cytochrome c oxidase
Lysyl oxidase
Superoxide dismutase
4
Alpha-2 globulin.
Functions:
Oxidizes Fe²⁺ → Fe³⁺
Facilitates iron binding to transferrin
Decreased in:
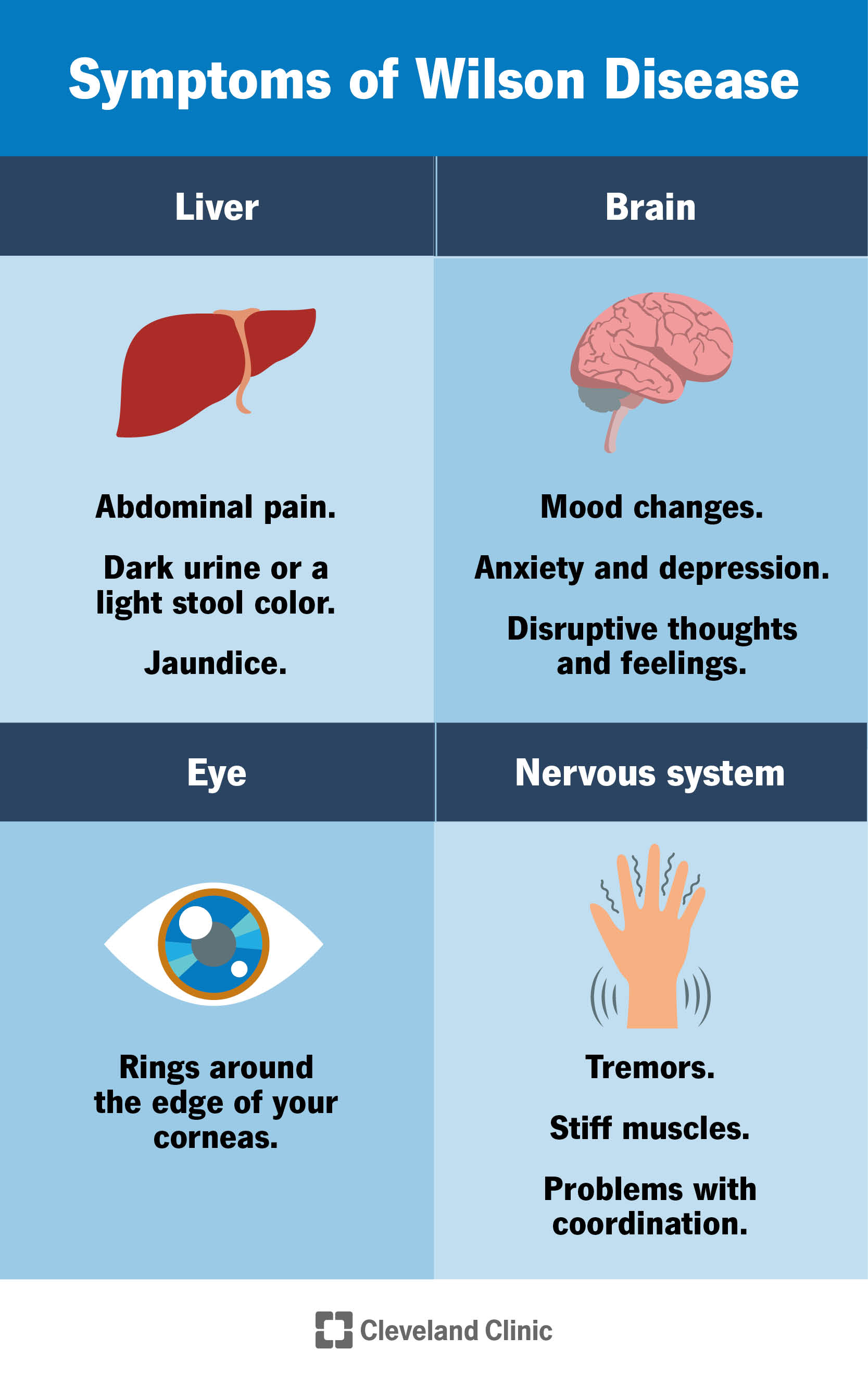
Wilson disease.
Copper accumulation in liver and brain.
Features:
Liver cirrhosis
Kayser-Fleischer rings
Neurological symptoms
Low ceruloplasmin.
Defective copper transport.
Features:
Kinky hair
Neurological deterioration
Required for synthesis of:
T3
T4
Stored in thyroid gland.
Deficiency leads to:
Goiter
Hypothyroidism
Cretinism (in children)

4
Functions:
DNA synthesis
Cell division
Wound healing
Immunity
Insulin storage
Enzyme component in:
Carbonic anhydrase
Alkaline phosphatase
Growth retardation
Hypogonadism
Delayed wound healing
Acrodermatitis enteropathica
Incorporated into:
Hydroxyapatite → Fluoroapatite.
Role:
Prevents dental caries
Strengthens enamel
Excess:
Dental fluorosis.
Component of:
Glutathione peroxidase.
Function:
Antioxidant
Thyroid hormone metabolism
Deficiency:
Keshan disease (cardiomyopathy).
Cofactor for:
Pyruvate carboxylase
Superoxide dismutase
Deficiency rare.
Excess:
Neurotoxicity.
Cofactor for:
Xanthine oxidase
Sulfite oxidase
Deficiency rare.
Component of:
Vitamin B12.
Not independently required apart from B12.
Trace role in:
Enzyme systems (minor role in humans).
Deficiency rare.
Enhances insulin action.
Part of:
Glucose tolerance factor.
Deficiency:
Impaired glucose tolerance.
Not essential nutrient.
Used pharmacologically in:
Bipolar disorder.
Toxicity:
Tremor, nephrotoxicity.
Copper → Iron metabolism
Ceruloplasmin → Ferrooxidase
Iodine → Thyroid hormones
Zinc → Growth & immunity
Fluoride → Teeth
Selenium → Antioxidant
Chromium → Insulin action
Cobalt → Vitamin B12
Q1. What is the normal role of copper in the body?
Iron metabolism, collagen cross-linking, antioxidant defense.
Q2. What plasma protein transports copper?
Ceruloplasmin.
Q3. What is the function of ceruloplasmin?
Oxidizes Fe²⁺ to Fe³⁺ for binding to transferrin.
Q4. Which disease is associated with low ceruloplasmin?
Wilson disease.
Q5. What are the main features of Wilson disease?
Liver cirrhosis, neurological symptoms, Kayser-Fleischer rings.
Q6. What is Menkes disease?
Defective copper transport leading to neurological deterioration and kinky hair.
Q7. What is the main function of iodine?
Synthesis of thyroid hormones (T3, T4).
Q8. Where is iodine stored?
Thyroid gland.
Q9. What is goiter?
Enlargement of thyroid due to iodine deficiency.
Q10. What is cretinism?
Severe congenital hypothyroidism due to iodine deficiency.
Q11. What are the major functions of zinc?
DNA synthesis, cell division, immunity, wound healing.
Q12. Name one zinc-containing enzyme.
Carbonic anhydrase.
Q13. What is acrodermatitis enteropathica?
Inherited zinc absorption defect.
Q14. Features of zinc deficiency?
Growth retardation, delayed wound healing, hypogonadism.
Q15. What is the role of fluoride in teeth?
Forms fluoroapatite and prevents dental caries.
Q16. What is dental fluorosis?
Excess fluoride causing mottled enamel.
Q17. Selenium is a component of which enzyme?
Glutathione peroxidase.
Q18. What is the role of selenium?
Antioxidant and thyroid hormone metabolism.
Q19. What disease is associated with selenium deficiency?
Keshan disease (cardiomyopathy).
Q20. Name one manganese-dependent enzyme.
Pyruvate carboxylase.
Q21. What happens in manganese excess?
Neurotoxicity.
Q22. Name one molybdenum-dependent enzyme.
Xanthine oxidase.
Q23. Is molybdenum deficiency common?
No, it is rare.
Q24. What is the biological role of cobalt?
Component of Vitamin B12.
Q25. Does cobalt have an independent function apart from B12?
No.
Q26. Is nickel essential in humans?
Its role is minimal and not clearly defined.
Q27. What is the main function of chromium?
Enhances insulin action.
Q28. What happens in chromium deficiency?
Impaired glucose tolerance.
Q29. Is lithium an essential nutrient?
No.
Q30. What is lithium used for clinically?
Treatment of bipolar disorder.
Q31. Name one toxicity feature of lithium.
Tremor.
Q32. Which trace element deficiency causes neurological and hepatic manifestations?
Copper deficiency or Wilson disease (copper excess).
Q33. Which trace element is important for thyroid hormone synthesis?
Iodine.
Q34. Which trace element is important in antioxidant defense along with glutathione?
Selenium.
Q35. Which trace element improves insulin sensitivity?
Chromium.
Q36. Which trace element deficiency causes growth retardation?
Zinc deficiency.
Q37. Which mineral protects against dental caries?
Fluoride.
Q38. Which trace element abnormality is seen in Wilson disease?
Copper accumulation with low ceruloplasmin.
Q39. Which trace element forms part of Vitamin B12?
Cobalt.
Q40. Which trace element excess can cause neurotoxicity?
Manganese.
Copper → Iron metabolism
Ceruloplasmin → Ferrooxidase
Iodine → Thyroid hormone
Zinc → Growth & immunity
Fluoride → Teeth
Selenium → Antioxidant
Chromium → Insulin action
Cobalt → B12
A. Transferrin
B. Albumin
C. Ceruloplasmin
D. Ferritin
A. Iron storage protein
B. Ferrooxidase
C. Hemoglobin
D. Hormone
A. Hemochromatosis
B. Wilson disease
C. Thalassemia
D. Pernicious anemia
A. Iron deficiency
B. Wilson disease
C. Zinc deficiency
D. Fluorosis
A. Iron excess
B. Defective copper transport
C. Zinc deficiency
D. Selenium toxicity
A. Insulin
B. Thyroid hormones
C. Cortisol
D. Growth hormone
A. Copper
B. Zinc
C. Iodine
D. Chromium
A. Rickets
B. Cretinism
C. Pellagra
D. Scurvy
A. Hemoglobin
B. Carbonic anhydrase
C. Collagen
D. Albumin
A. Hyperthyroidism
B. Growth retardation
C. Iron overload
D. Polycythemia
A. Copper
B. Zinc
C. Selenium
D. Manganese
A. Hydroxyapatite
B. Fluoroapatite
C. Ferritin
D. Hemoglobin
A. Goiter
B. Dental fluorosis
C. Hemolysis
D. Cirrhosis
A. Catalase
B. Glutathione peroxidase
C. Superoxide dismutase
D. Transferrin
A. Keshan disease
B. Wilson disease
C. Beriberi
D. Rickets
A. Pyruvate carboxylase
B. Hemoglobin
C. Thyroxine
D. Collagen
A. Xanthine oxidase
B. Hexokinase
C. Lactate dehydrogenase
D. Pepsin
A. Hemoglobin
B. Vitamin B12
C. Insulin
D. Collagen
A. Thyroid function
B. Insulin action
C. Collagen synthesis
D. Iron absorption
A. Hypothyroidism
B. Impaired glucose tolerance
C. Anemia
D. Bleeding
A. Epilepsy
B. Bipolar disorder
C. Diabetes
D. Hypertension
A. Hypoglycemia
B. Tremor
C. Goiter
D. Jaundice
A. DNA replication
B. Iron oxidation
C. Clotting
D. Thyroid hormone synthesis
A. Iron storage
B. Iron transport
C. Iron oxidation
D. Iron excretion
A. Copper deficiency
B. Copper accumulation
C. Iron overload
D. Zinc deficiency
A. Wound healing
B. Clotting
C. Myelin formation
D. Thyroid hormone synthesis
A. Thyroid hormone metabolism
B. Hemoglobin synthesis
C. Insulin secretion
D. Bone formation
A. Zinc
B. Selenium
C. Fluoride
D. Nickel
A. Zinc
B. Copper
C. Manganese
D. Fluoride
A. Zinc
B. Chromium
C. Nickel
D. Lithium
A. Has major metabolic role
B. Is part of hemoglobin
C. Has minimal defined role
D. Causes anemia
A. T3
B. T4
C. TSH
D. Insulin
A. Microcytic anemia
B. Polycythemia
C. Hypercalcemia
D. Hypothyroidism
A. Zinc
B. Copper
C. Selenium
D. Chromium
A. Dental caries
B. Rickets
C. Pellagra
D. Hemochromatosis
A. Brain
B. Heart
C. Liver
D. Kidney
A. Glucose tolerance factor
B. Hemoglobin
C. Collagen
D. Ceruloplasmin
A. Iron
B. Copper
C. Zinc
D. Fluoride
A. Thyroid hormone synthesis
B. DNA polymerase activity
C. Hemoglobin oxygen binding
D. Collagen hydroxylation
A. Ceruloplasmin
B. Ferritin
C. Transferrin
D. Catalase
A. Zinc and copper
B. Iodine
C. Fluoride
D. Nickel
A. Parkinsonism
B. Anemia
C. Rickets
D. Hypothyroidism
A. Peroxidase
B. Transferrin
C. Catalase
D. Hexokinase
A. Skeletal
B. Reproductive
C. Respiratory
D. Renal
A. Hypoglycemia
B. Liver damage
C. Hypothyroidism
D. Fluorosis
A. Collagen synthesis
B. Antioxidant defense
C. Clotting
D. Iron transport
A. Zinc
B. Selenium
C. Fluoride
D. Nickel
A. Thyroid
B. Liver
C. Kidney
D. Bone marrow
A. Selenium
B. Iodine
C. Zinc
D. Copper
A. Iron
B. Vitamin B12
C. Zinc
D. Copper
C
B
B
B
B
B
C
B
B
B
B
B
B
B
A
A
A
B
B
B
B
B
B
C
B
A
A
B
C
A
C
C
A
B
A
B
A
B
B
A
A
A
A
B
B
B
A
B
B
B
Q1. What is the main function of copper in the body?
Iron metabolism, collagen cross-linking, antioxidant defense, melanin synthesis.
Q2. Which plasma protein transports copper?
Ceruloplasmin.
Q3. What is the function of ceruloplasmin?
Oxidizes Fe²⁺ to Fe³⁺ to allow binding with transferrin.
Q4. What happens to ceruloplasmin levels in Wilson disease?
They decrease.
Q5. What is the basic defect in Wilson disease?
Impaired copper excretion leading to copper accumulation.
Q6. What are Kayser-Fleischer rings?
Copper deposition in cornea.
Q7. What is Menkes disease?
Defective copper transport causing deficiency symptoms.
Q8. Which copper-dependent enzyme is involved in collagen cross-linking?
Lysyl oxidase.
Q9. What is the biological role of iodine?
Synthesis of thyroid hormones T3 and T4.
Q10. Where is iodine stored?
Thyroid gland.
Q11. What hormone increases in iodine deficiency?
TSH.
Q12. What is goiter?
Enlargement of thyroid gland due to chronic TSH stimulation.
Q13. What is cretinism?
Severe congenital hypothyroidism due to iodine deficiency.
Q14. Which enzyme helps organification of iodine?
Thyroid peroxidase.
Q15. Name one important zinc-containing enzyme.
Carbonic anhydrase.
Q16. What are the main functions of zinc?
DNA synthesis, growth, immunity, wound healing.
Q17. What are features of zinc deficiency?
Growth retardation, hypogonadism, delayed wound healing.
Q18. What is acrodermatitis enteropathica?
Inherited defect in zinc absorption.
Q19. Zinc deficiency affects which system prominently?
Reproductive and immune systems.
Q20. What is the role of fluoride in teeth?
Forms fluoroapatite, increases resistance to caries.
Q21. What is dental fluorosis?
Excess fluoride causing mottled enamel.
Q22. Selenium is a component of which enzyme?
Glutathione peroxidase.
Q23. What is the role of glutathione peroxidase?
Reduces hydrogen peroxide and prevents oxidative damage.
Q24. What disease is associated with selenium deficiency?
Keshan disease.
Q25. Selenium also participates in which endocrine function?
Thyroid hormone metabolism (deiodinase enzymes).
Q26. Name one manganese-dependent enzyme.
Pyruvate carboxylase.
Q27. What happens in manganese excess?
Neurotoxicity resembling Parkinsonism.
Q28. Name one molybdenum-dependent enzyme.
Xanthine oxidase.
Q29. Is molybdenum deficiency common?
No, it is rare.
Q30. What is the biological role of cobalt?
Component of Vitamin B12.
Q31. Does cobalt have an independent metabolic function?
No, its role is via B12.
Q32. Is nickel essential in humans?
Its role is minimal and not clearly defined.
Q33. What is the main role of chromium?
Enhances insulin action.
Q34. Chromium is part of which factor?
Glucose tolerance factor.
Q35. What happens in chromium deficiency?
Impaired glucose tolerance.
Q36. Is lithium an essential trace element?
No.
Q37. What is lithium used for clinically?
Treatment of bipolar disorder.
Q38. Name one sign of lithium toxicity.
Tremor.
Q39. Why is lithium monitoring important?
Narrow therapeutic index and nephrotoxicity risk.
Q40. Which trace element links mineral metabolism with iron metabolism?
Copper (via ceruloplasmin).
Q41. Which trace element deficiency leads to hypothyroidism?
Iodine deficiency.
Q42. Which trace element is most important for wound healing?
Zinc.
Q43. Which trace element acts as antioxidant via enzyme system?
Selenium.
Q44. Which trace element is directly involved in insulin sensitivity?
Chromium.
Q45. Which trace element disorder causes liver cirrhosis and neurological signs?
Wilson disease (copper overload).
Get the full PDF version of this chapter.