Login
Welcome back! Please enter your details.
or
Don't have an account? Register here
Create Account
Join MedMentorEdu and start your medical journey.
or
Already have an account? Login here
Enhance your knowledge with our comprehensive guide and curated study materials.

Thyroid hormones are iodinated derivatives of tyrosine.
Two major hormones:
Thyroxine (T₄) – major secretory product
Triiodothyronine (T₃) – more biologically active
Synthesized and stored in the thyroid follicles.
Bound to plasma proteins in circulation:
Thyroxine-binding globulin (TBG)
Free hormone is biologically active.

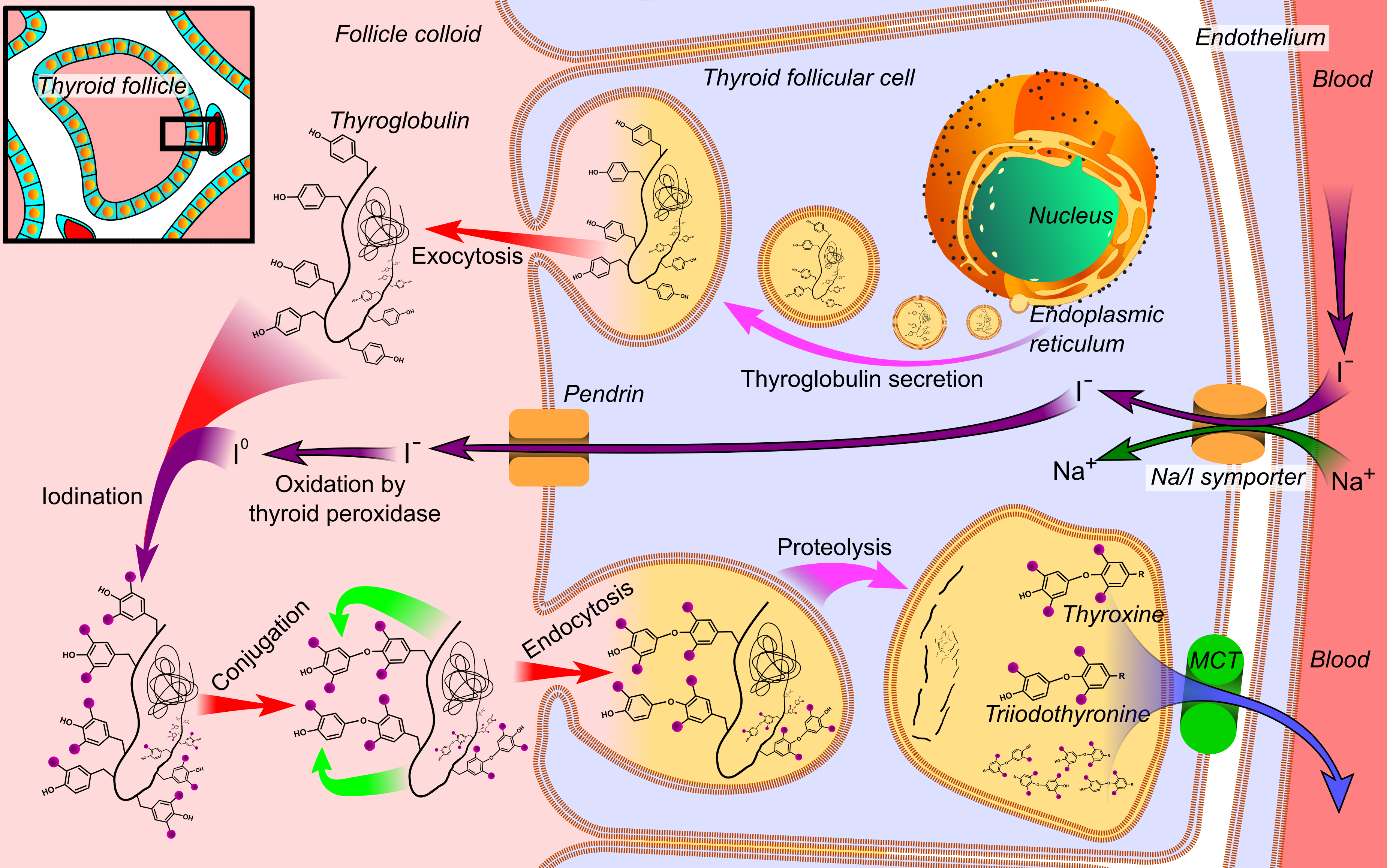
Occurs in thyroid follicular cells and colloid.
Requires iodine.
Iodide trapping
Active transport of iodide into follicular cell.
Oxidation of iodide
Iodide → iodine by thyroid peroxidase.
Organification
Iodine binds tyrosine residues of thyroglobulin.
Forms MIT and DIT.
Coupling reaction
MIT + DIT → T₃
DIT + DIT → T₄
Storage
Hormones stored in colloid as thyroglobulin.
Release
Proteolysis releases T₃ and T₄ into blood.
TSH stimulates all steps.

T₄ is secreted in greater quantity than T₃.
In peripheral tissues:
T₄ → T₃ by 5′-deiodinase.
Transported bound to:
TBG
Albumin
Transthyretin
Only free T₃ and T₄ are biologically active.
Thyroid hormones are lipophilic.
Enter cells by diffusion.
T₄ converted to T₃ inside cell.
T₃ binds to nuclear thyroid hormone receptor.
Hormone-receptor complex binds DNA at thyroid response elements.
Alters gene transcription and protein synthesis.
Action is slow in onset but long-lasting.


Thyroid hormones increase basal metabolic rate (BMR).
↑ Glucose absorption
↑ Glycolysis
↑ Gluconeogenesis
↑ Lipolysis
↓ Serum cholesterol
↑ Fatty acid oxidation
Physiological levels → ↑ protein synthesis
Excess → protein catabolism
↑ Oxygen consumption
↑ Heat production
Cardiovascular → ↑ heart rate, ↑ cardiac output
Nervous system → alertness, reflexes
Growth & development → brain maturation
GIT → ↑ appetite and motility
Musculoskeletal → normal bone growth
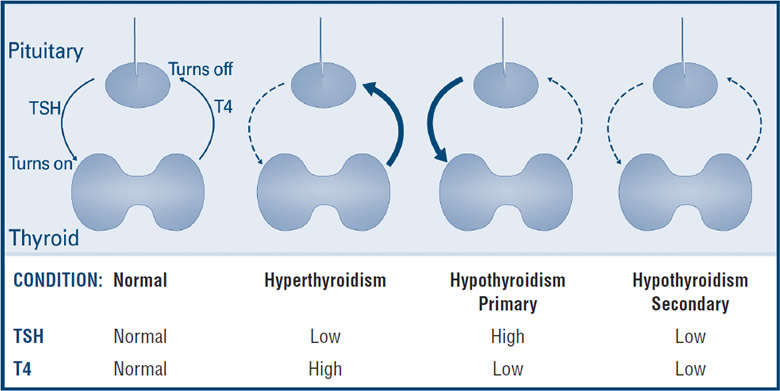
TRH (hypothalamus) → stimulates TSH
TSH (pituitary) → stimulates thyroid hormone synthesis
Negative feedback by T₃ and T₄ on TRH and TSH.
T₃ is 3–5 times more potent than T₄.
Thyroid hormones are stored in colloid.
Thyroid peroxidase is essential for synthesis.
Nuclear receptor–mediated action.
Increase BMR and oxygen consumption.
Essential for growth and CNS development.
Thyroid function is assessed by evaluating hormone levels, regulation, and gland activity.
Most sensitive screening test
↑ TSH → primary hypothyroidism
↓ TSH → hyperthyroidism
Reflects pituitary response to circulating thyroid hormones
Total T₄ and T₃ measure bound + free hormone
Free T₄ and free T₃ reflect biologically active hormone
T₃ rises earlier in hyperthyroidism
Thyroxine-binding globulin (TBG)
Alter total hormone levels but not free hormone
Measures iodine trapping and hormone synthesis
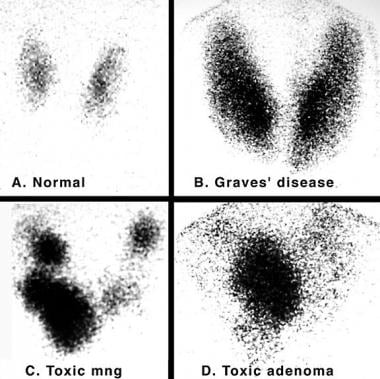
↑ Uptake → Graves disease
↓ Uptake → Thyroiditis
Anti-TPO antibodies → autoimmune thyroid disease
Anti-thyroglobulin antibodies
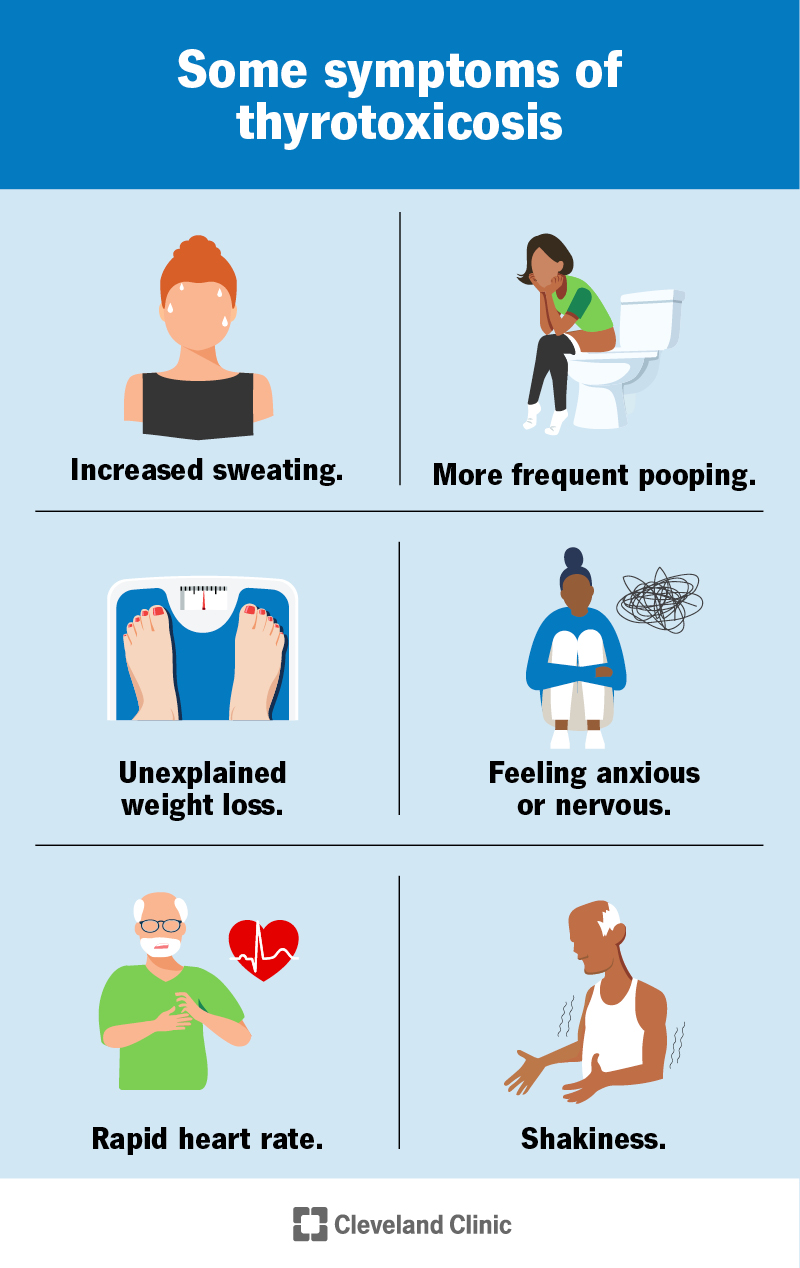
Hyperthyroidism is a state of excess thyroid hormone action.
Graves disease (most common)
Toxic multinodular goiter
Thyroid adenoma
Excess thyroid hormone intake
↓ TSH
↑ Free T₄ and/or T₃
↑ Radioiodine uptake (except thyroiditis)
Weight loss despite increased appetite
Heat intolerance
Sweating
Palpitations
Tachycardia
Tremors
Anxiety
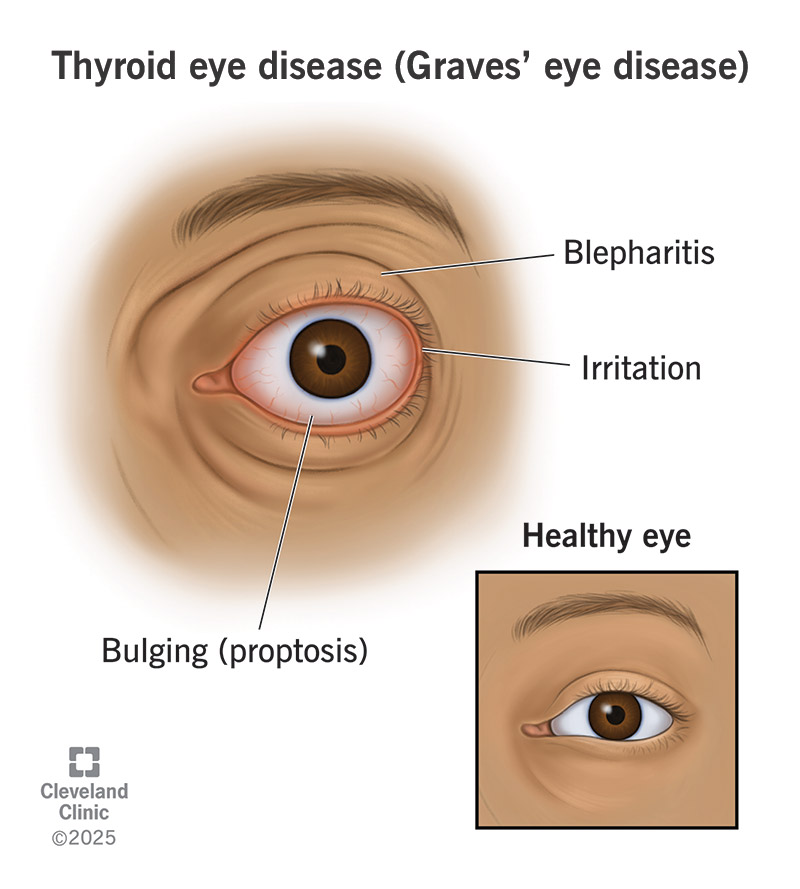
Goiter
Exophthalmos (Graves disease)
↑ Basal metabolic rate
↑ Lipolysis
↑ Protein catabolism

Hypothyroidism is a state of deficient thyroid hormone action.
Hashimoto thyroiditis (most common)
Iodine deficiency
Thyroidectomy
Drugs (antithyroid drugs)
Congenital absence of thyroid
↑ TSH (primary hypothyroidism)
↓ Free T₄
Normal or low T₃
Weight gain
Cold intolerance
Fatigue
Constipation
Bradycardia
Dry skin
Hair loss
Depression
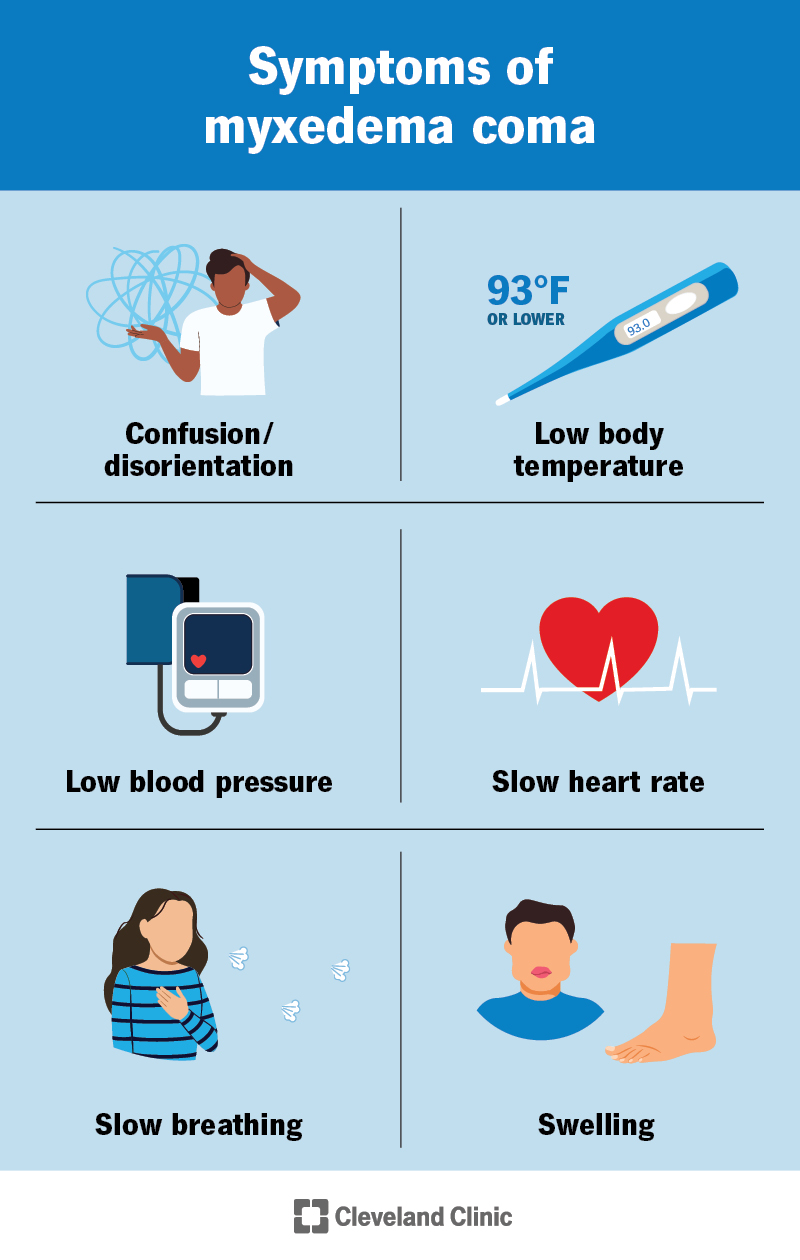
Puffy face (myxedema)
Cretinism (children)
Mental retardation
Growth failure
Myxedema (adults)
Non-pitting edema
Hypothermia
Reduced metabolism
| Feature | Hyperthyroidism | Hypothyroidism |
|---|---|---|
| TSH | ↓ | ↑ |
| T₃ / T₄ | ↑ | ↓ |
| BMR | Increased | Decreased |
| Weight | Loss | Gain |
| Heat tolerance | Decreased | Increased |
| Heart rate | Increased | Decreased |
TSH is the best screening test
T₃ toxicosis → early hyperthyroidism
Graves disease → autoimmune hyperthyroidism
Hashimoto thyroiditis → autoimmune hypothyroidism
Iodine deficiency → hypothyroidism
Thyroid hormones regulate BMR and growth
Serum TSH.
Because it reflects the pituitary response to circulating thyroid hormones.
The biologically active fraction of thyroid hormones.
Due to changes in thyroxine-binding globulin (TBG) levels.
To assess iodine trapping and thyroid hormone synthesis.
Hyperfunctioning thyroid (e.g., Graves disease).
Thyroiditis or exogenous thyroid hormone intake.
Anti-thyroid peroxidase (anti-TPO) and anti-thyroglobulin antibodies.
A clinical state of excess thyroid hormone action.
Graves disease.
↓ TSH, ↑ free T₄ and/or T₃.
Hyperthyroidism with elevated T₃ and normal T₄.
Weight loss, heat intolerance, palpitations, tremors, anxiety.
Due to increased basal metabolic rate.
Autoimmune inflammation of retro-orbital tissues.
A condition of deficient thyroid hormone action.
Hashimoto thyroiditis.
↑ TSH, ↓ free T₄.
Severe adult hypothyroidism with non-pitting edema.
Congenital hypothyroidism causing mental retardation and growth failure.
Due to decreased metabolic rate.
Because ACTH levels are not elevated.
They are increased.
Tachycardia and increased cardiac output.
Bradycardia and reduced cardiac output.
They are essential for normal CNS development and growth.
Leads to hypothyroidism and goiter.
Elevated TSH with normal T₃ and T₄.
Low TSH with normal T₃ and T₄.
They help diagnose, classify, and monitor thyroid disorders accurately.
A. Total T₄
B. Free T₄
C. Serum TSH
D. Radioiodine uptake
Answer: C
A. Total T₄
B. Protein-bound T₄
C. Free T₄ and Free T₃
D. Thyroxine-binding globulin
Answer: C
A. Graves disease
B. Hypothyroidism
C. Increased TBG
D. Thyroiditis
Answer: C
A. Subacute thyroiditis
B. Thyroid hormone overdose
C. Graves disease
D. Hypopituitarism
Answer: C
A. Graves disease
B. Toxic multinodular goiter
C. Thyroiditis
D. Iodine deficiency
Answer: C
A. Toxic adenoma
B. Thyroiditis
C. Graves disease
D. Iodine excess
Answer: C
A. ↑ TSH, ↓ T₄
B. ↓ TSH, ↑ T₄
C. ↑ TSH, ↑ T₄
D. ↓ TSH, ↓ T₄
Answer: B
A. Increased T₄ only
B. Increased T₃ with normal T₄
C. Increased TSH
D. Decreased T₃
Answer: B
A. Hashimoto thyroiditis
B. Subacute thyroiditis
C. Graves disease
D. Iodine deficiency goiter
Answer: C
A. Decreased appetite
B. Decreased metabolism
C. Increased basal metabolic rate
D. Malabsorption
Answer: C
A. Iodine deficiency
B. Hashimoto thyroiditis
C. Thyroid adenoma
D. Pituitary tumor
Answer: B
A. ↓ TSH, ↓ T₄
B. ↑ TSH, ↓ T₄
C. ↓ TSH, ↑ T₄
D. Normal TSH, ↓ T₄
Answer: B
A. Congenital hypothyroidism
B. Severe adult hypothyroidism
C. Hyperthyroid crisis
D. Thyroid cancer
Answer: B
A. Adult hypothyroidism
B. Hyperthyroidism in infancy
C. Congenital hypothyroidism
D. Pituitary insufficiency
Answer: C
A. Hypertension
B. Precocious puberty
C. Mental retardation
D. Hyperglycemia
Answer: C
A. Decreased
B. Normal
C. Increased
D. Unchanged
Answer: C
A. Hyperthyroidism
B. Graves disease
C. Hypothyroidism
D. Thyroid storm
Answer: C
A. Normal TSH with low T₄
B. High TSH with normal T₄
C. Low TSH with normal T₄
D. Low TSH with low T₄
Answer: B
A. ↑ TSH, normal T₄
B. ↓ TSH, normal T₄
C. ↑ TSH, ↑ T₄
D. ↓ TSH, ↓ T₄
Answer: B
A. Only adult metabolism
B. Only reproductive function
C. Growth and CNS development
D. Electrolyte balance only
Answer: C
A 28-year-old woman presents with weight loss, palpitations, heat intolerance, and tremors. Her pulse is 110/min. Laboratory tests show low TSH and elevated free T₄.
Question:
What is the most likely diagnosis?
Answer:
Hyperthyroidism
A patient has hyperthyroid symptoms with low TSH, high T₃, and normal T₄.
Question:
What is this condition called?
Answer:
T₃ toxicosis
A 32-year-old woman presents with goiter and protrusion of eyes. Radioactive iodine uptake is increased.
Question:
What is the most likely cause?
Answer:
Graves disease
A patient with thyrotoxic symptoms has low radioactive iodine uptake.
Question:
What is the most likely diagnosis?
Answer:
Thyroiditis or exogenous thyroid hormone intake
A patient has increased total T₄ but normal free T₄ and normal TSH.
Question:
What is the likely explanation?
Answer:
Increased thyroxine-binding globulin (TBG)
A 45-year-old woman complains of weight gain, cold intolerance, constipation, and fatigue. Examination shows dry skin and bradycardia. TSH is elevated.
Question:
What is the diagnosis?
Answer:
Primary hypothyroidism
A patient with hypothyroidism shows high anti-thyroid peroxidase antibodies.
Question:
What is the most likely cause?
Answer:
Hashimoto thyroiditis
A patient with pituitary tumor has low TSH and low T₄.
Question:
What type of hypothyroidism is this?
Answer:
Secondary hypothyroidism
A newborn presents with large tongue, hypotonia, and delayed milestones.
Question:
Which thyroid disorder explains these features?
Answer:
Congenital hypothyroidism (cretinism)
A child with untreated hypothyroidism develops severe mental retardation.
Question:
Why does this occur?
Answer:
Because thyroid hormones are essential for normal CNS development.
A patient presents with non-pitting edema of face and extremities, hypothermia, and bradycardia.
Question:
What is this condition called?
Answer:
Myxedema
A patient shows elevated TSH with normal T₃ and T₄ levels.
Question:
What is the diagnosis?
Answer:
Subclinical hypothyroidism
A patient has low TSH with normal thyroid hormone levels.
Question:
What is this condition termed?
Answer:
Subclinical hyperthyroidism
A hyperthyroid patient develops atrial fibrillation.
Question:
Which metabolic effect of thyroid hormone explains this?
Answer:
Increased β-adrenergic sensitivity and cardiac output
A patient with hypothyroidism has elevated serum cholesterol.
Question:
Why does this occur?
Answer:
Due to reduced LDL receptor activity and decreased lipid metabolism.
A patient with hyperthyroidism experiences muscle weakness and weight loss.
Question:
Which metabolic effect is responsible?
Answer:
Increased protein catabolism
A woman treated with excess levothyroxine shows suppressed TSH.
Question:
What does this indicate?
Answer:
Iatrogenic hyperthyroidism
A patient has goiter with normal thyroid hormone levels.
Question:
What is this condition called?
Answer:
Euthyroid goiter
A patient with iodine deficiency develops goiter.
Question:
Why does goiter occur despite low thyroid hormone levels?
Answer:
Due to TSH-mediated thyroid hyperplasia.
A hyperthyroid patient complains of excessive sweating and heat intolerance.
Question:
Which hormone effect explains this?
Answer:
Increased basal metabolic rate and heat production
Serum TSH
Free T₃ and Free T₄
Thyroxine (T₄)
Triiodothyronine (T₃)
Thyroxine-binding globulin (TBG)
Thyroid peroxidase
Radioactive iodine uptake (RAIU)
Graves disease
Thyroiditis or exogenous hormone intake
Graves disease
TSH receptor antibody
Autoimmune inflammation of retro-orbital tissues
↓ TSH, ↑ T₃/T₄
High T₃ with normal T₄
Increased basal metabolic rate
Tachycardia
Hashimoto thyroiditis
Anti-thyroid peroxidase antibody
↑ TSH, ↓ T₄
Severe adult hypothyroidism
Glycosaminoglycan deposition
Congenital hypothyroidism
Bradycardia
Hypercholesterolemia
↑ TSH with normal T₃/T₄
↓ TSH with normal T₃/T₄
Essential for normal brain maturation
Hypothalamic-pituitary-thyroid axis
T₃ and T₄
Chronic TSH stimulation
Serum TSH
Get the full PDF version of this chapter.